
























Coksartrosis- This is arthrosis of the hip joint.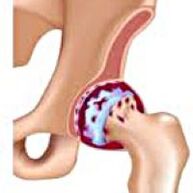 It develops gradually, for several years, prone to progression, can be both one -sided and double -sided.It is accompanied by pain and restriction of movements in the joint.In the later stages, atrophy of the hip muscles and shortening of the limb are observed.The diagnosis is established on the basis of clinical symptoms and radiography results.In the early stages of coxarthrosis, conservative treatment.With the destruction of the joint, especially in patients of young and middle age, surgery (endoprosthetics) is indicated.
It develops gradually, for several years, prone to progression, can be both one -sided and double -sided.It is accompanied by pain and restriction of movements in the joint.In the later stages, atrophy of the hip muscles and shortening of the limb are observed.The diagnosis is established on the basis of clinical symptoms and radiography results.In the early stages of coxarthrosis, conservative treatment.With the destruction of the joint, especially in patients of young and middle age, surgery (endoprosthetics) is indicated.
General information
Coksartrosis (osteoarthrosis or deforming arthrosis of the hip joint) is a degenerative-dystrophic disease.It usually develops at the age of 40 years and older.It may be a result of various injuries and joint diseases.Sometimes it occurs for no apparent reason.Coksartrosis is characterized by a gradual progressive course.In the early stages, conservative methods of treatment are used.In the later stages, the joint function can only be restored operational.
In orthopedics and traumatology, coxarthrosis is one of the most common arthrosis.The high frequency of its development is due to a significant load on the hip joint and the widespread prevalence of congenital pathology - joint dysplasia.Women suffer from coksartrosis a little more often than men.
The causes of coksartrosis
The primary (arising for unknown reasons) and secondary (developed as a result of other diseases) arthrosis of the hip joint are distinguished.
Secondary coksartrosis can be the result of the following diseases:
- Hip joint dysplasia.
- Inborn dislocation of the thigh.
- Pertes's diseases.
- Aseptic necrosis of the thigh head.
- Infectious lesions and inflammatory processes (for example, arthritis of the hip joint).
- Injuries (traumatic dislocations, fractures of the hip neck, pelvic fractures).
Coksartrosis can be either one -sided or double -sided.With primary coxarthrosis, a concomitant lesion of the spine (osteochondrosis) and knee joint (gonartrosis) is often observed.
Risk factors
Among the factors that increase the likelihood of the development of coxarthrosis include:
- Constant increased load on the joint.Most often observed in athletes in people with an excess body weight.
- Circulatory disorders, hormonal changes, metabolic disorders.
- Pathology of the spine (kyphosis, scoliosis) or stop (flat feet).
- Elderly and senile age.
- A sedentary lifestyle.
Coksartrosis itself is not inherited.However, certain features (metabolic disorders, skeleton structural features and the weakness of cartilage) can be inherited by the child from parents.Therefore, in the presence of blood relatives suffering from coxarthrosis, the probability of the occurrence of the disease is slightly increased.
Patanatomy
The hip joint is formed by two bones: ileum and femoral.The head of the thigh is articulated with the acetabulum of the iliac bone, forming a peculiar “hinge”.During movements, the acetabulum remains motionless, and the femoral head moves in various directions, ensuring flexion, extension, abduction, bringing and rotational hips.
During movements, the articular surfaces of the bones unhindered slide relative to each other, thanks to the smooth, elastic and durable hyalin cartilage covering the cavity of the swivel cavity and the head of the thigh.In addition, hyaline cartilage performs a shock -absorbing function and is involved in the redistribution of the load during movement and walking.
In the joint cavity there is a small amount of joint fluid, which plays the role of lubrication and provides nutrition of hyaline cartilage.The joint is surrounded by a dense and strong capsule.Above the capsule are large femoral and gluteal muscles, which provide movements in the joint and, along with hyalin cartilage, are also shock absorbers that protect the joint from injuries with unsuccessful movements.
With coxarthrosis, the joint liquid becomes thicker and more viscous.The surface of the hyaline cartilage dries, loses smoothness, covered with cracks.Due to the roughness that has arisen, the cartilage during movements is constantly injured about each other, which causes their thinning and aggravates pathological changes in the joint.As coxarthrosis progresses, the bones begin to deform, “adapting” to increased pressure.The metabolism in the joint is deteriorating.In the later stages of coxarthrosis, severe atrophy of the muscles of the sore limb is observed.
Symptoms of coxarthrosis
The main symptoms of the disease include pain in the joint, inguinal region, thigh and knee joint.Also, with cokesartrosis, stiffness of movements and stiffness of the joint, gait disturbance, lameness, atrophy of the hip muscles and shortening of the limb on the side of the lesion are observed.A characteristic feature of coksartrosis is a restriction of abduction (for example, the patient is difficult when trying to sit down on a chair).The presence of certain signs and their severity depends on the stage of coxarthrosis.The first and most constant symptom is pain.
AtCoksartrosis of the 1st degreePatients complain of periodic pain, which occurs after physical activity (running or prolonged walking).The pain is localized in the joint, less often in the thigh or knee.After rest, it usually disappears.The gait for coxarthrosis of the 1st degree is not broken, the movements are preserved in full, there is no muscle atrophy.
On the X -ray of the patient suffering from coxarthrosis of the 1st degree, mild changes are determined: moderate uneven narrowing of the joint gap, as well as bone growths around the external or internal edge of the acetabulum in the absence of changes from the head and neck of the femur.
AtCoksartrosis 2 degreesThe pain becomes more intense, often appear at rest, radiates into the thigh and groin.After significant physical activity, the patient with coksartrosis begins to limp.The volume of movements in the joint decreases: the abduction and internal rotation of the thigh is limited.
In X -ray images for coxarthrosis of the 2nd degree, significant uneven narrowing of the joint gap (more than half from normal height) is determined.The femoral head is somewhat shifted upward, deformed and increases in size, and its contours become uneven.Bone growths with this degree of coxarthrosis appear not only on the internal, but also on the outer edge of the acetabulum and go outside the cartilage.
AtCoksartrosis 3 degreesThe pain becomes constant, worry of patients not only during the day, but also at night.Walking is difficult, when moving, a patient with coksartrosis is forced to use a cane.The volume of movements in the joint is sharply limited, the muscles of the buttock, hips and lower legs are atrophied.The weakness of the removing muscles of the thigh becomes the cause of the deviation of the pelvis in the front plane and shortening the limb on the sore side.In order to compensate for shortening, a patient suffering from coksartrosis, when walking, tilts the body to the sore direction.Because of this, the center of gravity shifts, the load on the sore joint increases sharply.
On radiographs for coxarthrosis of the 3rd degree, a sharp narrowing of the joint gap, a pronounced expansion of the thigh head and multiple bone growths are detected.
Diagnostics
The diagnosis of coxarthrosis is based on clinical signs and data of additional studies, the main of which is radiography.In many cases, x -rays make it possible to establish not only the degree of coxarthrosis, but also the cause of its occurrence.So, for example, an increase in the neck-diaphyseal angle, the scenes and flattening of the acetabulum indicate dysplasia, and changes in the shape of the proximal part of the femur are indicated that coksartrosis is a consequence of Pertes's disease or youthful epiphysiolysis.On radiographs of patients with coxarthrosis, changes can also be detected indicating injuries.
As other methods of instrumental diagnosis of coxarthrosis, CT and MRI can be used.Computed tomography allows you to study pathological changes in detail by bone structures in detail, and magnetic resonance imaging provides the opportunity to evaluate disorders by soft tissues.

Differential diagnosis
First of all, coxarthrosis should be differentiated from gonarthrosis (osteoarthrosis of the knee joint) and osteochondrosis of the spine.Atrophy of muscles, which occurs at 2 and 3 stages of coxarthrosis, can cause pain in the knee joint, which are often expressed brighter than pain in the area of damage.Therefore, with the patient’s complaints about the knee pain, a clinical (inspection, palpation, determination of the volume of movements) is the study of the hip joint, and if coxarthrosis is suspected, to direct the patient to radiography.
Pain for radicular syndrome (compression of nerve roots) for osteochondrosis and some other diseases of the spine can imitate pain with coxarthrosis.Unlike coksartrosis, when squeezing the roots, the pain occurs suddenly, after an unsuccessful movement, a sharp turn, lifting weights, etc., is localized in the buttock area and spreads along the back of the thigh.A positive symptom of tension is detected - severe pain when the patient tries to raise a straightened limb, lying on his back.At the same time, the patient freely takes his leg to the side, while in patients with coksartrosis, the abduction is limited.It should be borne in mind that osteochondrosis and coksartrosis can be observed at the same time, therefore, in all cases, a thorough examination of the patient is necessary.
In addition, cokesartrosis is differentiated with trochanteritis (boot burgit) - aseptic inflammation in the area of attachment of the gluteal muscles.Unlike coxarthrosis, the disease develops rapidly, within 1-2 weeks, usually after an injury or significant physical activity.The intensity of pain is higher than with coksartrosis.Limitations of movements and shortening of the limb are not observed.
In some cases, with an atypical course of the disease or reactive arthritis, symptoms resembling coxarthrosis can be observed.Unlike coxarthrosis, with these diseases, the peak of pain falls on night.The pain syndrome is very intense, can decrease when walking.The morning stiffness is characteristic, which occurs immediately after waking up and gradually disappears within a few hours.
Treatment of coxarthrosis
Treatment of pathology is engaged in traumatologist orthopedists.The choice of treatment methods depends on the symptoms and stage of the disease.At 1 and 2 stages of coxarthrosis, conservative therapy is carried out.During the period of exacerbation of coxarthrosis, injection blocks, non -steroidal anti -inflammatory drugs (pyroxes, indomethacin, diclofenac, ibuprofen, etc.) are used.It should be borne in mind that drugs of this group are not recommended for a long time, since they can have a negative effect on the internal organs and suppress the ability of hyalin cartilage to restore.
To restore damaged cartilage for coksartrosis, funds from a group of chondroprotectors (chondroitin sulfate, cartilage extract, etc.) are used.To improve blood circulation and eliminate spasm of small vessels, vasodilating drugs (zinnarisine, nicotine acid, pentoxifillin, xanthinol nicotinate) are prescribed.According to the indications, muscle relaxants are used (muscle relaxation drugs).
With stubborn pain syndrome, patients suffering from coksartrosis can be prescribed intra -articular injections using hormonal drugs (hydrocortisone, triamcinolone, metrumor).Treatment with steroids must be carried out with caution.In addition, with coxarthrosis, local products are used - warming ointments that do not have a pronounced therapeutic effect, however, in some cases they relieve muscle spasm and reduce pain due to their “distracting” action.Also, with coxarthrosis, physiotherapeutic procedures are prescribed (luminous, ultrasonic therapy, laser treatment, UHF, inductothermia, magnetotherapy), massage, manual therapy and therapeutic gymnastics.
The diet for coksartrosis does not have an independent therapeutic effect and is used only as a means to reduce weight.Reducing body weight allows you to reduce the load on the hip joints and, as a result, facilitate the course of coksartrosis.In order to reduce the load on the joint, the doctor, depending on the degree of coxarthrosis, may recommend to walk with a cane or crutches.
In the later stages (with coxarthrosis of the 3rd degree), the only effective method of treatment is the operation - replacing the destroyed joint with an endoprosthesis.Depending on the nature of the lesion, either single -pole (replacing only the head of the thigh) or two -pole (replacing both the head of the thigh and the swivel cavity) can be used.
The operation of endoprosthetics for coxarthrosis is carried out in a planned manner, after a complete examination, under general anesthesia.In the postoperative period, antibiotic therapy is carried out.The seams are removed on 10-12 days, after which the patient is prescribed for outpatient treatment.After endoprosthetics, rehabilitation measures are necessarily held.
In 95% of cases, surgical intervention to replace the joint with coxarthrosis ensures a complete restoration of the limb function.Patients can work, actively move and even play sports.The average service life of the prosthesis, subject to all recommendations, is 15-20 years.After this, a second operation is required to replace a worn endoprosthesis.